
(also known as Cerebral Vasculitis)
Updated in August 2025 by Claire M Rice, Associate Professor in Neuroinflammation and Honorary Consultant Neurologist, University of Bristol and North Bristol NHS Trust, Bristol, UK
What is Central Nervous System Vasculitis?
Inflammation is a normal response to tissue injury but, when out of proportion to the triggering insult and/or is misdirected to normal tissues, then damage to the structure and function of the affected tissue occurs.
Vasculitis is inflammation targeted against blood vessels. The inflammatory process within the vessel wall leads to vessel damage, with viable degrees of blockage and haemorrhage which cause downstream injury and disruption to the function of tissues and organs.
Central nervous system (CNS) vasculitis refers to involvement of the brain (cerebral vasculitis) and/or spinal cord by inflammation of the supplying blood vessels. It may occur in association with vasculitis affecting other tissues and organs (secondary vasculitis) or, less commonly, there may be no evidence of vasculitis outside the CNS. When no recognised trigger for vasculitis affecting the CNS can be identified (such as infection or another neuroinflammatory disease), it is referred to as primary CNS vasculitis or primary angiitis of the CNS (PACNS).
Who is affected?
Primary CNS vasculitis is considered a rare disease. The exact number of people affected is not known but is estimated to be 2.4 per million per year. Males may be slightly more likely to have the condition than females. Typically, the onset occurs in people in their 50s, but people of any age can be affected, including children.
What causes CNS vasculitis?
Some causes of CNS vasculitis are recognised to be triggered by infections e.g. tuberculosis, varicella zoster and hepatitis viruses), cancers (e.g. lymphoma), drugs (cocaine and amphetamines) or other immune mediated conditions e.g. rheumatoid arthritis and sarcoidosis). In some people, the immune system spontaneously directs an attack on the brain and spinal cord, and it is not fully understood why this occurs.
What are the symptoms?
The symptoms of CNS vasculitis can be very different from one person to another. People may experience fatigue, headache, changes in behaviour or personality with confusion and/or memory impairment, seizures, limb weakness and balance problems, impaired control of bowel and/or bladder function, difficulties with hearing and vision and reduced consciousness/coma. Some experience only a few symptoms whilst others have many. Symptoms typically emerge over weeks and months, although sometimes they can occur more quickly and, occasionally, people may become critically unwell.
Making a diagnosis

Vasculitis affecting the CNS can be difficult to diagnose because many of the symptoms overlap with those of other neuroinflammatory conditions, such as multiple sclerosis or neurosarcoidosis. Although investigations are often abnormal, they may not show a particular pattern that allows them to be clearly distinguished from other more common conditions. For this reason, the diagnosis may be delayed and some people with CNS vasculitis may have been given an incorrect diagnosis initially. In some cases, it can take several months or even years for the diagnosis to be made.
Investigations that are likely to be considered when someone is suspected of having CNS vasculitis include blood tests (which may be normal) and imaging of the brain and/or spinal cord. People will often have both CT and MRI, with dedicated imaging of the vessels (angiogram and/or vessel wall imaging). Although there are many reasons why brain vessels can be abnormal, these tests can be helpful if they detect changes. However, the vasculature can still appear normal on current imaging of the brain and spinal if the smallest vessels are affected; this is because the vessels are below the resolution limits of the scan.
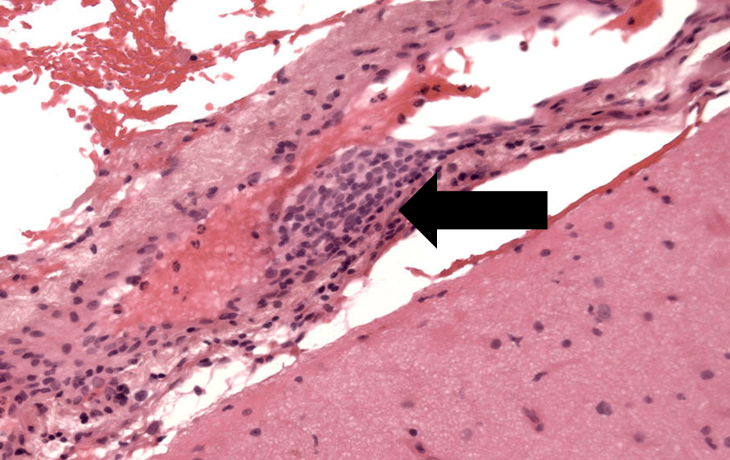
The definitive way to make the diagnosis of vasculitis in any organ is to sample tissue (biopsy) and demonstrate inflamed vessels using a microscope. When the condition affects the brain and/or spinal cord in isolation, this is challenging due to the surgical risks associated with the procedure. However, depending on the location of the biopsy, it can often be done safely. Surgical targeting of an area that is abnormal on imaging, increases the likelihood of getting a biopsy result that is informative, but this isn’t always possible.
Treatment
In CNS vasculitis for which a trigger has not been identified, the rationale underlying treatment is to dampen down the overactive immune system and stop the misdirected attack on the brain and/or spinal cord. As with other types of serious vasculitis, high doses of steroids are often required; these work relatively quickly compared to other forms of immune therapies but, unfortunately, can be associated with significant side effects. Treatments are usually thought about as either ‘induction’ treatments where the aim is to get control of the condition quickly, and ‘maintenance’ therapy to prevent recurrence (or ‘relapse’).
Cyclophosphamide is commonly used induction therapy which aims to ‘reset’ the immune system, although other therapies e.g. rituximab, are sometimes considered. Longer term immunosuppression is usually also required as maintenance therapy e.g. methotrexate, azathioprine or mycophenolate; one of these therapies is likely to be required for several years. More information on the drugs prescribed for CNS vasculitis is available in the Glossary of Drugs and Side Effects.
Prognosis
Relapse occurs in about a quarter of cases. With correct treatment the prognosis is much better than in the past.
Research
Due to the relative rarity of the condition, there have not been clinical trials undertaken in CNS vasculitis. However, researchers continue to work towards improving understanding of how and why the condition arises, as well as to optimise diagnosis and management.
Key points
- PACNS is very rare
- Organs involved include the brain and spinal cord
- Symptoms are non-specific and may develop over a long period of time
- Treatment depends on disease severity.
- Additional research to improve speed and accuracy of diagnosis, as well as optimal treatment pathways is required urgently.
Further reading
Biopsy-proven PACNS: results from the large, multicentre cohort of cerebral vasculitis patients
The diagnosis of primary central nervous system vasculitis
Personal stories
The personal story of a patient with CNS vasculitis (from 2016) can be viewed at: Viv’s story