
Dr Alina Casian (Nephrology) Thomas and Guys Hospital, London Supported by
Professor David D’Cruz, Consultant Rheumatologist (Lupus & Connective Tissue Disease) Thomas & Guys Hospital, London
February 2016
What is Immunoglobulin G4 Disease?
IgG4-RD is a recently recognised, rare autoimmune condition that can affect most organs and links a number of inflammatory diseases that previously were considered unrelated and affecting only one organ.
It is caused by cells in the blood producing harmful substances that attack the body’s own tissues to cause inflammation, swelling / lumps and scarring.
IgG4-RD can cause many different symptoms and may affect one or several organs at the same time or at different times.
Although symptoms may sometimes be mild, it can also cause severe organ damage and even death if not treated.
IgG4-RD can affect the eyes, retroperitoneum (inside of the belly around the aorta, the largest blood vessel), pancreas, gallbladder, kidneys, lungs, tear and salivary glands, thyroid, meninges (lining of the brain), testicles, prostate etc.
Who are affected?
IgG4-RD usually occurs most commonly in middle-aged and older men, especially if the kidneys, pancreas or retroperitoneum are involved. However, those patients with IgG4-RD affecting their eyes or salivary glands are equally likely to be male or female.
What is the aetiology (cause)?
The cause of IgG4-RD is unclear. IgG4 is a type of antibody found in the blood of all people and is part of the immune system (body’s defences). Some people with IgG4-RD have high levels of IgG4 in the blood but the reason for this is not clear. Interestingly, IgG4 levels may also be raised in people who do not have IgG4-RD.
What are the symptoms?
IgG4-RD may present very differently amongst patients, depending on the various organs involved. Sometimes people have mild symptoms (such as tiredness, loss of appetite) for months or even years before seeking medical help.
Other common symptoms include:
- Eyes – swelling /lump, pain, loss of eyesight, redness
- Skin – lumps, rashes
- Lungs – breathlessness, wheeze, lump, cough
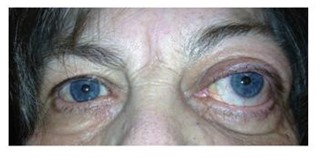

Inflammation of the left lacrimal (tear) gland 
Diagnosis
As IgG4-RD often presents in a similar way to other diseases (including cancer), making the diagnosis can be difficult and usually requires biopsy (sampling of the affected tissue). Some patients may have even had unnecessary operations in the past.
Blood tests usually show evidence of inflammation and raised IgG4 levels can support the diagnosis but are not specific enough by themselves.
The diagnosis will depend on the doctor recognising the pattern of clinical symptoms, blood and biopsy results.
After diagnosis, pictures taken using scans (CT, MRI, PET) can help clarify which other organs are affected, the severity of disease and the response to treatment.
Treatment
Prednisolone (steroid) is traditionally used first to achieve control of moderate IgG4-RD. If the patients do not fully respond to steroids, another treatment is added: methotrexate if the patient does not have kidney disease, otherwise azathioprine or mycophenolate mofetil.
The majority of patients respond well to these standard medicines. However, they have several side effects, especially steroids that can cause weight gain, high blood pressure, diabetes or osteoporosis (thinning of the bones).
Rituximab has also been used successfully to treat a selected, small group of patients already on standard medication whose IgG4-RD is not controlled or who experience harmful effects from treatment or remain dependent on high doses of steroids.
Rituximab works specifically by removing the harmful blood cells that make IgG4. It is usually given as 2 injections in the veins 2 weeks apart and, if IgG4-RD flares again, rituximab can be repeated after 6 months or longer.
Rituximab is being approved in the UK for use as 3rd choice treatment (after steroids +/- methotrexate/azathioprine/ mycophenolate mofetil) for a small number of patients with difficult-to-treat IgG4-RD, in order to prevent further scarring and organ damage.
Treatment specific to the affected organs may also be needed, such as:
- Thyroxine hormone replacement if the thyroid gland becomes underactive
- Insulin if the pancreas is affected by diabetes mellitus
What is the prognosis of IgG4-related disease?
The prognosis of IgG4-RD is variable and depends on the severity of disease and damage already done to major organs (especially kidneys, pancreas, aorta, liver). If IgG4-RD is diagnosed early, the inflammation can usually be controlled with treatment to prevent further damage.
IgG4-RD may spontaneously disappear, persist or flare from time to time, requiring a temporary increase in treatment.
The duration of treatment for patients with IgG4-RD is not clear and each case should be discussed individually with the doctors.
Key Points
- IgG4-RD is a rare autoimmune disease that may be present for months or even years before the actual diagnosis
- Diagnosis is often difficult as IgG4-RD may mimic other diseases including cancer
- Treatment depends on the severity of the disease
- Most patients respond well to standard treatment with steroids +/- methotrexate (or azathioprine or mycophenolate mofetil)
- Rituximab is beneficial for the small number of patients who do not respond sufficiently to standard treatment
- The disease may flare again after the initial treatment.
- Future studies are needed to clarify the best treatment